
{kind=link}
I’ve long lamented a certain blind spot among my fellow physicians and scientists, a problem that the COVID-19 pandemic has made even more painfully apparent to me. What I’m referring to is our inability as a group to recognize when science is being distorted and thereby weaponized in order to become disinformation. This is not a new technique, but it’s been turbocharged and used more frequently and intensely than ever before. I was reminded of this by a recent Twitter thread, the first part of which I will cite here:
McCullough just published a paper in “Food and Chemical Toxicology” that posits biological mechanisms underlying purported innate immune suppression and harm from SARS-CoV-2 mRNA vaccination, using VAERs to support their hypotheses of vaccine relatedness of noted pathologies.
— Prof Jeffrey S Morris (@jsm2334) April 21, 2022
This long review article presents many details about various biological pathways, but their links to mRNA vaccines are almost wholly speculative. In some cases, they link to other vaccines, old mRNA technology, or COVID-19 infection, but are not directly linked to mRNA vaccines.
— Prof Jeffrey S Morris (@jsm2334) April 21, 2022
Naturally, antivaxxers have been spreading this study far and wide as yet more “evidence” that mRNA vaccines against COVID-19 are dangerous:
Please tell me how to sue and how to get a lawyer before I die. I was 100% documented healthy and now I have an issue in almost every system in my body. My eyes can no longer focus, my brain is vibrating 24hrs a day, and I can no longer work or exercise.
— WeTheUSPeople (@WeTheUSPeople) April 23, 2022
Dear Helen u weren’t the premier who relentlessly pushed this dangerous injecticide down our throats. A lot of citizens are suffering ma’am. Time to pull the plug I think.
Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of… https://t.co/c9kP1r38aM
— Sagezza (@sagezza2) April 21, 2022
I could list many more such Tweets, as well as the study being shared this way on Facebook with similar messaging that it’s strong evidence that mRNA vaccines are dangerous and suppress the innate immune system, the spike protein is toxic, and large numbers of people are being harmed by them—exactly as intended by the antivaxxers who wrote it. But is it evidence of any of this? I think that you know the answer. Rather, it is a prime example of what I now refer to as misinformation (or disinformation) by scientific review article (or, more accurately, a pseudo-review article). It appears to have all the trappings of science, but its speculation goes far beyond what the science will support, all in the service of promoting a certain narrative and providing what seems to be scientific support for a pseudoscientific conspiracy theory. Unsurprisingly, it worked, as its social media engagement demonstrates.
It is also true that Prof. Morris nailed it perfectly in the fourth Tweet in his series. This “review” article is almost entirely speculative. However, not having such a long history of examining antivaccine pseudoscience, he missed observing that the article is speculative in a deceptive manner that I’ve seen many times before dating back to the Hannah Poling story in 2008, in which antivaxxers tried to rebrand autism as a mitochondrial disorder in which vaccines interacted with a metabolic disease to trigger autism, a narrative that “functional medicine” guru Dr. Mark Hyman echoed and that was still being promoted up to right before the pandemic. As a preview, I’ll mention that other examples include Yehuda Shoenfeld’s “ASIA” diagnosis, the idea of “molecular mimicry” by HPV vaccines, and “homologous recombinaltion tiniker” (misspelling preserved from the original). Think of this long “review” as a Gish gallop disguised as a review article. There are lots of claims, all speculative, many for which the cited evidence is at best tenuous and often requires quite the leap to go from what the evidence finds about a process and how that process might be related to COVID-19 vaccination.
Combined with the speculative claims about biological mechanism is also an exercise in dumpster diving into the Vaccine Adverse Events Reporting System (VAERS) database in a manner very much like how Tracy Beth Høeg and other COVID-19 contrarians did for myocarditis last summer in an echo of how Mark and David Geier did it 16 years ago trying to “prove” that mercury in the thimerosal preservative that was used in some childhood vaccines until around 2001-2 caused autism, other antivaxxers tried to link the H1N1 vaccine to miscarriages (sound familiar?), and how Stephanie Seneff used the same deceptive technique to try to demonstrate in 2012 that aluminum adjuvants in vaccines and exposure to acetaminophen caused autism. Since COVID-19 vaccines hit the scene in December 2020, weaponization of VAERS reports has been a constant among antivaxxers.
Who wrote this paper?
The last name I mentioned is important. Why? Because Stephanie Seneff is the lead author of the paper that’s been going around. She was an antivaxxer before the pandemic who blamed vaccines and GMOs for autism; it’s not surprising that she pivoted to being anti-COVID-19 vaccines, although early in the pandemic she tried to blame glyphosate and e-cigarettes for COVID-19. (I kid you not.) Like many antivaxxers before and during the pandemic, she has no primary expertise in vaccines, infectious disease, public health, epidemiology, or any other relevant biomedical academic disciplines. Rather, she’s a computer scientist at MIT, and her sole qualification (if you can call it that) is an undergraduate biophysics degree from the late 1960s. In addition to her history promoting antivaccine misinformation, she has also made some truly off-base proclamations over the last several years, including her prediction in 2014 that by 2025 half of all children born that year will be autistic. (It’s 2022 now. How’d that prediction work out?) She even once claimed that GMOs can cause concussions.
We’ve also met Peter McCullough before. He’s a cardiologist who has been promoting a narrative that COVID-19 vaccines are causing a “holocaust” for over a year now. Unsurprisingly, he’s also promoted ivermectin as a near “miracle cure” for COVID-19. Basically, Dr. McCullough has become a major force in promoting COVID-19 pseudoscience, quackery, and misinformation and is frequently on the speaker’s list for COVID-19 denial rallies and events.
I was interested in the other two authors, Greg Nigh and Anthony Kyriakopoulous, as I didn’t recall having heard of them before. Greg Nigh is listed as being affiliated with Immersion Health in Portland, OR. Surprise! Surprise! Immersion Health is a naturopathic oncology clinic:
Immersion Health opened its doors in 2014. Dr. Greg Nigh and Maria Zilka, the clinic’s founders, have collaborated on cancer treatment for 10 years. Immersion Health brings them together to offer intensive, comprehensive and individualized programs for the treatment of all types and stages of cancer. In addition to cancer care, Dr. Nigh offers the full range of primary care medicine, including functional lab testing and genetic polymorphism analysis.
Immersion Health was started as an intensive naturopathic oncology clinic. Dr. Nigh develops comprehensive and intensive treatment programs for all types and stages of cancer.
The cancer treatment approach at Immersion Health is unique, recognizing cancer as a metabolic disease. At Immersion Health we are delivering therapies that address all aspects of health and vitality, because long-term success against cancer depends on a strong immune system, low inflammation, ongoing detoxification, lifelong nutritional strategies, stress management, physical activity and much more. Immersion Health brings this all together into individualized treatment plans that optimize every individual’s potential for recovery and ongoing wellness.
Naturopathy is quackery, and naturopathic oncology doubly so. Just peruse this blog for many, many examples. Unsurprisingly, naturopaths have pivoted to COVID-19 quackery. Of the group, Anthony Kyriakopoulous has the closest to what one might consider actual qualifications, working at the Nasco AD Biotechnology Laboratory, a lab in Greece described as a “private research laboratory focusing on the discovery, development and thereafter clinical application of patented medicinal formulations to provide innovative technology against infections inflammation autoimmunity and cancer”. He also appears to have some expertise in RNAs and inflammation, but, as I always say, if you’re an expert in something but associate your name with cranks, quacks, and pseudoscientists like Stephanie Seneff, Peter McCullough, and Greg Nigh, that should be a major red flag that perhaps the expert has gone crank.
Of course, defenders of authors like these would call what I just wrote an “ad hominem” attack. It’s not, really. It could be an ad hominem attack if the only reason I gave for their paper being wrong were because it was authored by them, but you know me better than that. My response to such a charge is always the same: Qualifications matter. Author history matters. All but one of the authors are utterly unqualified to write a review article like this, and the one who arguably does have some qualifications is not the first author or the corresponding author. That tells me a lot before I read beyond the abstract.
Finally, this is a long article. That’s why, unlike Prof. Morris, I’m going to approach it more from the angle of disinformation and its similarities to previous papers like it before the pandemic than get into the weeds of each and every claim, especially given that he has provided a good blog post that does get into the weeds, some of which I will borrow from given that it’s impossible not to address some claims. Again, Prof. Morris was quite correct that the paper is largely speculative and doesn’t cite a lot of primary evidence, but that very speculativeness is a hallmark of many prior antivax narratives that try to postulate a biological “mechanism” by which vaccines caused autism and all manner of other health issues dating way, way back. Similarly, the paper does a VAERS dumpster dive to try to lend credibility to its speculation.
A scientific review as disinformation
One of the more interesting things, from a disinformation standpoint, is a figure right at the beginning of the review, described as a “graphical abstract.” When I first read the paper, I hadn’t recalled seeing such a figure described thusly, but I did recall a number of figures from the past in which vaccines were inserted into metabolic and immune pathways to make a science-y looking diagram arguing how vaccines caused this problem or other. Let’s take a look:
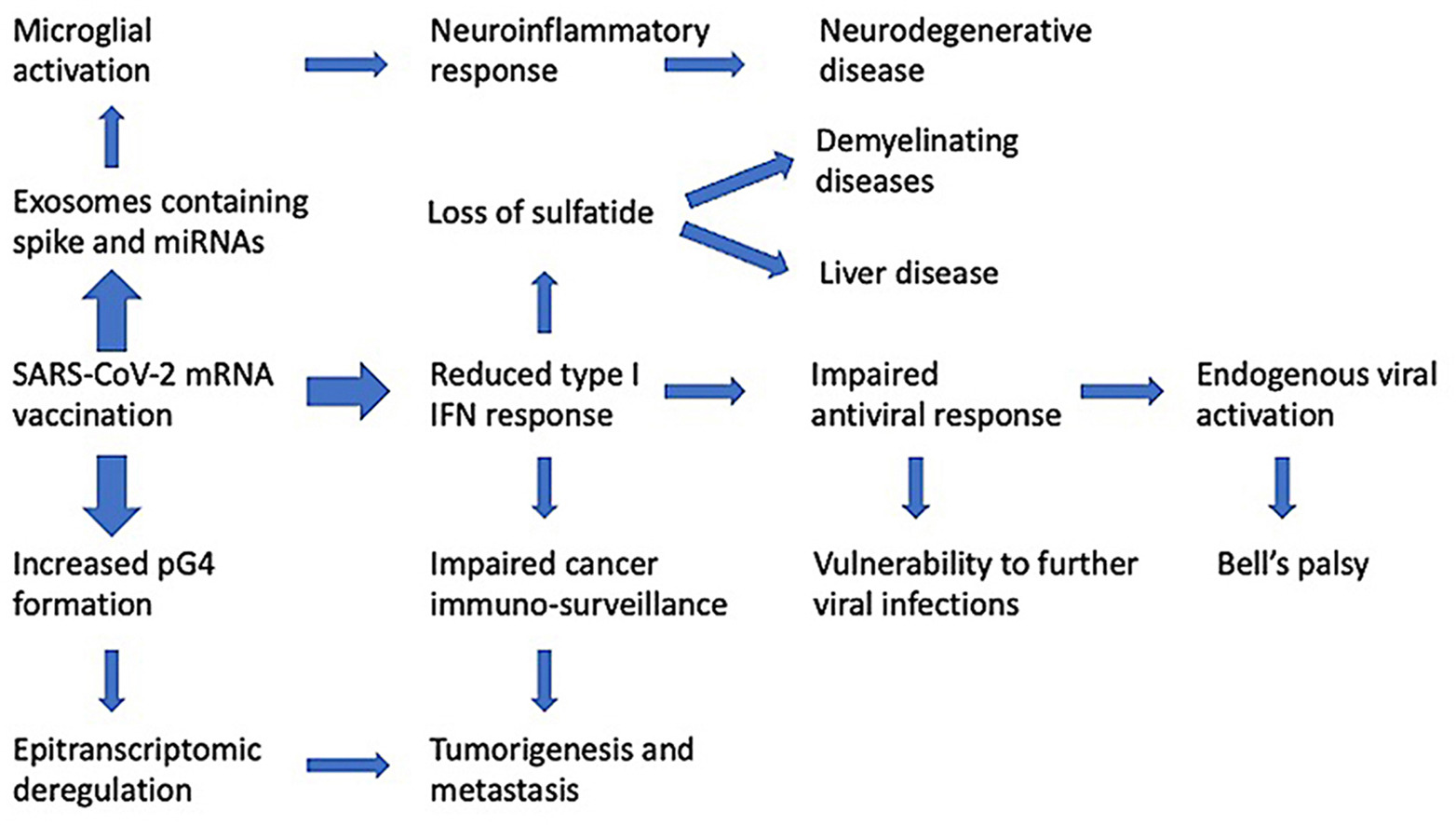
This “graphical abstract” looks so very, very scientific, doesn’t it?
Let’s look at the actual written abstract and compare:
The mRNA SARS-CoV-2 vaccines were brought to market in response to the public health crises of Covid-19. The utilization of mRNA vaccines in the context of infectious disease has no precedent. The many alterations in the vaccine mRNA hide the mRNA from cellular defenses and promote a longer biological half-life and high production of spike protein. However, the immune response to the vaccine is very different from that to a SARS-CoV-2 infection. In this paper, we present evidence that vaccination induces a profound impairment in type I interferon signaling, which has diverse adverse consequences to human health. Immune cells that have taken up the vaccine nanoparticles release into circulation large numbers of exosomes containing spike protein along with critical microRNAs that induce a signaling response in recipient cells at distant sites. We also identify potential profound disturbances in regulatory control of protein synthesis and cancer surveillance. These disturbances potentially have a causal link to neurodegenerative disease, myocarditis, immune thrombocytopenia, Bell’s palsy, liver disease, impaired adaptive immunity, impaired DNA damage response and tumorigenesis. We show evidence from the VAERS database supporting our hypothesis. We believe a comprehensive risk/benefit assessment of the mRNA vaccines questions them as positive contributors to public health.
I will concede that the immune response to the vaccine is likely different than the immune response to a SARS-CoV-2 infection, but not in the way described in this paper that implies that it’s just as bad or worse than the immune reaction to infection. The authors claim that the “mRNA vaccine initiates a set of biological events that are not only different from that induced by infection but are in several ways demonstrably counterproductive to both short- and long-term immune competence and normal cellular function” but, as Prof, Morris notes, they self-cite to do it:
A preprint has revealed a remarkable difference between the characteristics of the immune response to an infection with SARS-CoV-2 as compared with the immune response to an mRNA vaccine against COVID-19 (Ivanova et al., 2021).
Where does that link go? Straight back to this review article! (If you don’t believe me and think that I altered the link, just go to the article itself and click on the link.) The actual paper is a preprint from August that appears to be still a preprint, and the interesting thing about it is that the paper demonstrates a good thing about COVID-19 mRNA vaccines, namely:
In COVID-19 patients, immune responses were characterized by a highly augmented interferon response which was largely absent in vaccine recipients. Increased interferon signaling likely contributed to the dramatic upregulation of cytotoxic genes in the peripheral T cells and innate- like lymphocytes observed in COVID-19 patients. Analysis of B and T cell repertoires revealed that while the majority of clonal lymphocytes in COVID-19 patients were effector cells, in vaccine recipients clonal expansion was primarily restricted to circulating memory cells. Taken together, our analysis of immune responses to the mRNA vaccine reveals that despite the lack of dramatic inflammation observed during infection, the vaccine elicits a robust adaptive immune response.
Then Seneff et al. also claim:
All of these observations are consistent with the idea that the anti-COVID-19 vaccines actively suppress type I IFN signaling, as we will discuss below.
More likely, it’s consistent with the vaccines not stimulating type I IFN signaling and all the inflammation that comes with it, which is a good thing. After all, that’s what you want from a vaccine: a robust immune response that doesn’t come with all the inflammation caused by the infection but still ends up producing memory cells that can be reactivated by contact with the provoking antigen! After all, the main issue is that actual infection is, well, infection. It stimulates the immune response as the virus is replicating freely and damaging cells, thus leading to inflammation, both specific to the infection and nonspecific. Also, the mRNA vaccines induce muscle cells to make the SARS-CoV-2 spike protein, which is the protein that binds to the ACE2 receptor on human cells and allows the virus to enter them. That’s the target of the immune response. Infection would be expected to result in an immune response to more viral proteins than just the spike protein.
Just the introduction is full of additional misrepresentations, for example:
Since long-term pre-clinical and Phase I safety trials were combined with Phase II trials, then phase II and III trials were combined (Kwok, 2021); and since even those were terminated early and placebo arms given the injections, we look to the pharmacosurveillance system and published reports for safety signals. In doing so, we find that that evidence is not encouraging. The biological response to mRNA vaccination as it is currently employed is demonstrably not similar to natural infection. In this paper we will illustrate those differences, and we will describe the immunological and pathological processes we expect are being initiated by mRNA vaccination. We will connect these underlying physiological effects with both realized and yet-to-be-observed morbidities. We anticipate that implementation of booster vaccinations on a wide scale will amplify all of these problems.
This is a deceptive misrepresentation of what actually happened, something I wrote about over a year ago. Basically, once the vaccines were released under an emergency use authorization (EUA), there was no way to guarantee that subjects in the placebo arm of the large clinical trials carried out by Pfizer and Moderna for their vaccines would not simply get vaccinated. After all, the EUA had been issued, and doctors and the government were doing everything they could to encourage people to be vaccinated against COVID-19. The unblinding and crossover of the clinical trials was actually the ethical thing to do, even if it complicated the long term safety surveillance. Once a vaccine demonstrated to be effective and safe has been released to the public, regardless of the regulatory mechanism under which it was approved, it was, quite simply, unethical to continue to withhold the vaccine from the subjects in the placebo group. This is an issue that antivaxxers and those who enable them have long distorted; so it’s not at all surprising that Seneff et al. are doing it too.
They also parrot a number of common anti-COVID-19 vaccine talking points that I’ve discussed both here and at my not-so-super-secret other blog:
The mRNA vaccines manufactured by Pfizer/BioNTech and Moderna have been viewed as an essential aspect of our efforts to control the spread of COVID-19. Countries around the globe have been aggressively promoting massive vaccination programs with the hope that such efforts might finally curtail the ongoing pandemic and restore normalcy. Governments are reticent to consider the possibility that these injections might cause harm in unexpected ways, and especially that such harm might even surpass the benefits achieved in protection from severe disease. It is now clear that the antibodies induced by the vaccines fade in as little as 3–10 weeks after the second dose (Shrotri et al., 2021), such that people are being advised to seek booster shots at regular intervals (Centers for Disease Control and Prevention, 2021b). It has also become apparent that rapidly emerging variants such as the Delta and now the Omicron strain are showing resistance to the antibodies induced by the vaccines, through mutations in the spike protein (Yahi et al., 2021). Furthermore, it has become clear that the vaccines do not prevent transmission of the disease, but can only be claimed to reduce symptom severity (Kampf, 2021a). A study comparing vaccination rates with COVID-19 infection rates across 68 countries and 2947 counties in the United States in early September 2021, found no correlation between the two, suggesting that these vaccines do not protect from spread of the disease (Subramanian and Kumar, 2947). Regarding symptom severity, even this aspect is beginning to be in doubt, as demonstrated by an outbreak in an Israeli hospital that led to the death of five fully vaccinated hospital patients (Shitrit et al., 2021). Similarly, Brosh-Nissimov et al. (2021) reported that 34/152 (22%) of fully vaccinated patients among 17 Israeli hospitals died of COVID-19.
Note the appeal to “natural immunity” (more properly called postinfection immunity or infection-induced immunity) above all, even though evidence is increasingly showing that “natural immunity” wanes as well and likely doesn’t last much longer than vaccine-induced immunity. Moreover, the rise of the very variants that can evade prior immunity (Delta and Omicron) demonstrates that “natural immunity” can be bypassed by the virus almost as easily as vaccine-induced immunity. In addition, as any immunologist knows, antibody levels don’t stay high forever after an infection or a vaccine. If that were the case, our blood would soon become a viscous glop of nothing but high levels of antibodies to previously-encountered antigens to which the immune system had responded. It’s the development of memory cells, which can quickly be reactivated to produce antibodies when the immune system encounters an antigen again, that matter more. As for disease transmission, once again we see the “Nirvana fallacy”, in which anything less than 100% safety and efficacy implies that a treatment or vaccine is worthless, in this case that the “vaccine doesn’t prevent transmission”. Actually, it does; it’s just not 100% effective and the effect, like that of the vaccine, does wane. The way to look at it is that the vaccines are “less good” at preventing infection and transmission than they are at preventing serious disease and death, not that they don’t prevent transmission or infection at all. Let’s just say that it doesn’t look good when the evidence cited for the claim that the “vaccines don’t prevent transmission” is a study as risibly awful as Subramanian and Kumar.
The rest of the paper before the VAERS dumpster diving reminds me of something I used to do with a friend of mine back when we were in junior high. It probably won’t surprise readers to learn that, even at that tender age, I was a science geek (also just what was considered in the mid-1970s to be just a geek). There were times when my friend and I would wildly speculate about science that we only slightly understood, wondering if there were a link between this idea and other ideas, whether genetic engineering were possible (remember, this was the 1970s), and a whole bunch of “what ifs”. It was fun at the time, even though our knowledge of science was junior high science geek level, and such flights of speculative fancy no doubt increased our enthusiasm for science, to the point where both of us became doctors, me a surgeon-scientist and my friend a pathologist.
Let’s just say a lot of this paper reminds me of those days, stringing ideas together without much in the way of good evidence, and saying “What if?” Of course, junior high science geeks ultimately grew up to study serious science, but this paper strikes me as being similar to what we did, the exception being that we were engaging in our speculative arguments innocently. This paper is not so innocent, even if it seems to have applied a gloss of scientific findings to the same sort of speculative flights of fancy. For instance, the authors try to claim that this “suppression” of IFN responses predisposes people to cancer:
Both IFN-α and IRF9 are also apparently necessary for the cancer-preventative properties of a fully functional BRCA2 gene. In a study presented as an abstract at the First AACR International Conference on Frontiers in Basic Cancer Research, Mittal and Chaudhuri (2009) describe a set of experiments which show for the first time that BRCA2 expression leads to increased IFN-α production and augments the signal transduction pathway resulting in the complexing of IRF9, STAT1 and STAT2 described previously. Two years prior, Buckley et al. (2007) had established that BRCA1 in combination with IFN-γ promotes type I IFNs and subsequent production of IRF7, STAT1, and STAT2. Thus, the exceedingly important cancer regulatory genes BRCA1 and BRCA2 rely on IRF7 and IRF9, respectively, to carry out their protective effects. Rasmussen et al. (2021) reviewed compelling evidence that deficiencies of either IRF7 or IRF9 lead to significantly greater risk of severe COVID-19 illness. Importantly, they also note that evidence suggests type I IFNs play a singularly important role in protective immunity against COVID-19 illness, a role that is shared by multiple cytokines in most other viral illnesses including influenza.
Being a breast cancer surgeon, I know a fair amount about BRCA2 and BRCA1, as well as their functions preventing cancer. Also note how Seneff et al. cite a 13-year-old abstract about BRCA2 and IFN-α production. If I were reviewing the paper, I would have asked: Where’s the published paper? I would have noted that, given that this is a 13-year-old finding, it should have found its way into the scientific literature by now. A quick search of PubMed for anything published together by the two authors who published the abstract about BRCA2 showed me that apparently these results never made it into a full paper. Even if they had, the abstract itself simply showed that the BRCA2 tumor suppressor was needed for breast cells to make IFN-α. In other words, the finding is basically irrelevant to COVID-19 vaccines or any other vaccines. If the result held up, it would really only show that the need for BRCA2 to produce IFN-α in breast cells might be relevant to the cancer suppressing function of the gene. In fairness, more recent data suggest a link between BRCA2 deficiency and immune signaling, but that leaves the question: Why did Seneff et al. so selectively cite a 13-year-old abstract?
Then there’s this:
A recent early-release study has found that the mRNA in the COVID-19 vaccines is present in germinal centers in secondary lymphoid tissue long after the vaccine is administered, and that it continues to synthesize spike glycoprotein up to at least sixty days post-vaccination (Röltgen et al., 2022). This suggests that immune cells taking up the mRNA in the arm muscle migrate into the lymph system to the lymph nodes, presumably in order to expose B-cells and T-cells to the toxic antigen. The persistence of the mRNA in the lymph nodes and its sustained synthesis of SARS-CoV-2 spike glycoprotein reflect the clever engineering involved in the mRNA technology, as described above.
Imagine that! The antigen sticks around in the lymph nodes to stimulate an immune response! How horrible!
This paper is rife with such odd citations about biological processes, many unrelated to vaccination or infection, all marshaled in the service of trying to convince you that mRNA-based COVID-19 vaccines cause harm. Indeed, the authors even invoke codon usage, fear mongering about “coinfection” with other viruses, and supposed molecular mimicry (although they don’t use the term) of the spike protein because of its supposed similarity to various important human proteins. There are mentions of microRNAs (something in which I have some expertise as well) and exosomes, as well as metabolism. Rather than go through them all (or even a lot of them), I’m going to quote Prof. Morris:
This very long review article presents many details about various biological pathways, most related to cancer, but their links to mRNA vaccines are almost wholly speculative. In some cases, they link to other vaccines, old mRNA technology, or COVID-19 infection, but are not directly linked to mRNA vaccines.
In fact, so much of their evidence is from papers on severe COVID-19 infections, not vaccination, much of the evidence in this article might be better suited to a paper pointing out potential downstream dangers of severe COVID-19 infections than on trying to raise alarm about mRNA vaccination.
A number of places in the article seem to make stronger statements linking mRNA vaccines to some of these processes, but they self-cite a previous review article by senior author McCullough and do not reference any primary biological research making these connections.
They suggest connections of these mechanisms to various anecdotal case reports for herpes zoster reactivation, liver damage, optic neuropathy, T cell lymphoma progression, Hepatitis C reactivation, events not yet confirmed to be related to mRNA vaccination.
The paper amounts to laying out a series of hypotheses about mechanisms of harm that may come from mRNA vaccines. Hypothesis generation is a valuable exercise, including in this context of understanding downstream biological effects of vaccination that might induce harm.
However, not all hypotheses are equally supported. Some are well-girded in direct evidence from relevant studies, while others are more speculative and extrapolate principles from other settings, e.g. SARS-CoV-2 infections or other injected vaccines, as done here.
Again, Prof. Morris is entirely too kind. I would put it a different way. This “review” is the scientific equivalent of a form of what the kids like to call shitposting – a bunch of low-quality provocative assertions on social media designed to provoke a visceral reaction. In this case, the visceral reaction intended is disgust and fear of mRNA-based COVID-19 vaccines. Prof. Morris is, of course, quite correct when he identifies the purpose of this torrent of speculation as shifting the burden of proof, with the authors claiming that their wild speculation must be taken seriously by scientists and their proposed harms be investigated right now, rather than presenting anything resembling actual compelling evidence why their ill-formed hypotheses should be taken seriously in the context of what is already well-established about human biology and immunology:
Challenging public health institutions to disprove the assertions made by this article, rather than taking responsibility to validate them or urge other scientists to do so, is a bold move. This type of statement in which one makes a claim and presumes it should assumed true unless other scientists can disprove it, is the classic “shifting the burden of truth” trick. A scientist proposing a hypothesis has the burden of validating it; it is not the responsibility of the scientific community to disprove it, and the hypothesized claim certainly does not have the benefit of presumption of truth unless disproven. This is a common tactic used by many during the pandemic.
In addition, this whole “review” article is one big Gish gallop, in which a torrent of questionable claims is made in an attempt to overwhelm the reader with the quantity of claims, with no regard for their quality. I’ve been told that it’s impossible to Gish gallop in a paper, because one has the time to read and address every claim, but one could easily spend 20,000 words or more to address each and every claim in this “review”. That’s the point. That’s why I’m trying to point out how this review is similar previous efforts and to put it into context with disinformation in general
The purpose of a paper like this is to put a seemingly scientific gloss on speculative scientific bafflegab in which the various concepts are at least “six degrees of separation” away from any biological “framework” having anything to do with vaccines. Scientists with the requisite expertise recognize this handwaving as the crap that it is, but those without the requisite expertise don’t. Even some doctors and scientist without the proper specialized expertise won’t recognize it for what it is, disinformation.
After all the scientific shitposting (if you’ll excuse the term), Seneff et al. then try to make all their speculation and JAQing off sound plausible by appealing to—you guessed it!—VAERS.
Into the VAERS dumpster!
Let’s take a look at the VAERS reports examined by Seneff et al. The easiest thing for me to do is to quote the Tweets. For example, here’s Table I, which Seneff attribute to inflammation:
One nerve inflammation symptom is anosmia. They claim this “clearly demonstrates” the spike injected into arm reached the olfactory nerve, ignoring that anosmia is common with COVID-19 but not linked to vaccine, and could be caused by previous COVID-19 infection, not vaccine. pic.twitter.com/M7WBiENxI3
— Prof Jeffrey S Morris (@jsm2334) April 21, 2022
Indeed. There is no known mechanism by which the tiny amounts of spike protein that make it into the bloodstream after vaccination could injure the olfactory bulb and cause anosmia (loss of the sense of smell), which also happens to be a well-known symptom of COVID-19 infection itself. There’s also quite a bit of evidence that it is direct infection of the cells in the olfactory bulb with SARS-CoV-2 that is responsible for anosmia. If there’s a symptom of the virus that we’d expect the vaccine not to cause, it would be anosmia.
Let’s just say that this passage from the review should tell you all you want to know about it. I laughed out loud when I read it:
There were nearly 100,000 cases of nausea or vomiting, which are common symptoms of vagus nerve stimulation or damage (Babic and Browning, 2014). 14,701 cases of syncope linked to COVID-19 vaccines represented 96.3% of all cases of syncope, a well-established feature of vagus nerve dysfunction (Fenton et al., 2000).
People passed out after vaccination, and that must mean the vaccine was somehow hurting the vagus nerve? Seriously, I can only laugh. Lots of people faint after blood draws or shots; it’s a common reaction, particularly in certain populations. It’s the same sort of claim that, you might remember, antivaxxers made about the HPV vaccine because so many teenage girls faint after receiving it, except that they at least had a more plausible mechanism than that the vaccine somehow messed up the vagus nerve. Don’t get me wrong. Stimulation of the vagus nerve can cause fainting. That’s why they call it a “vasovagal” reaction. However, in general it’s pain or fear that results in that stimulation.
Since I’m a cancer doctor, I’ll mention this one too:
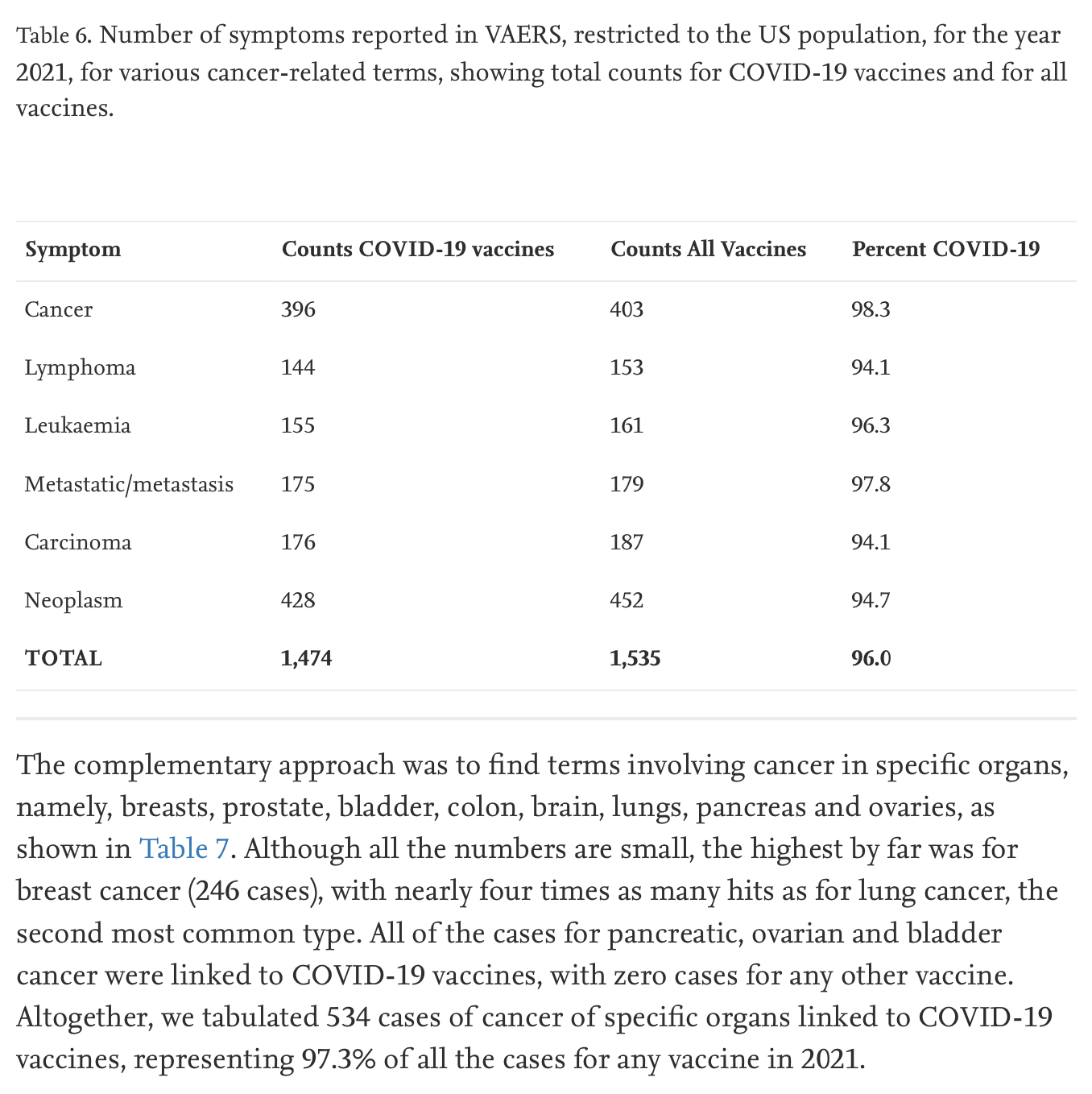
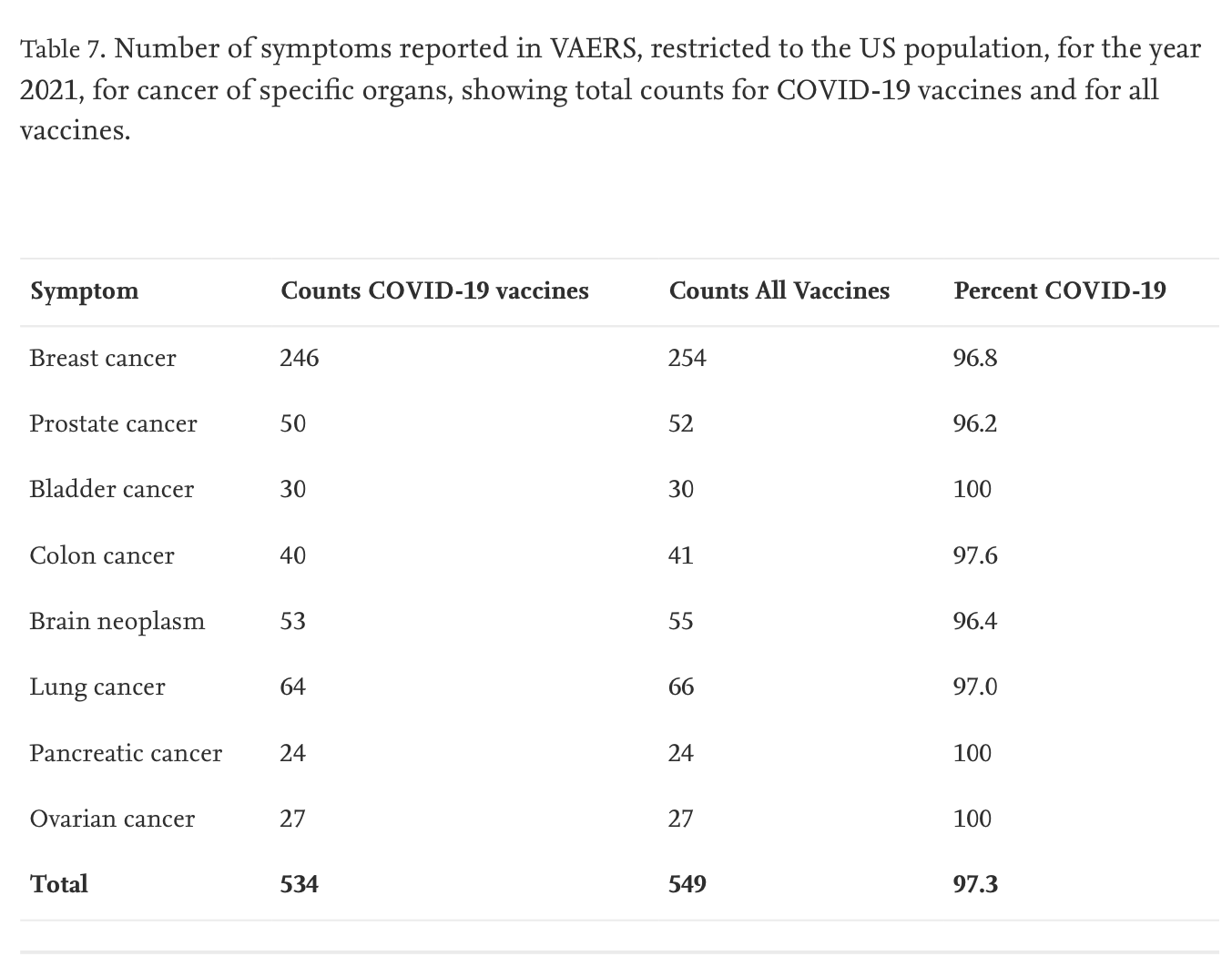
The authors even admit:
Cancer is a disease generally understood to take months or, more commonly, years to progress from an initial malignant transformation in a cell to development of a clinically recognized condition. Since VAERS reports of adverse events are happening primarily within the first month or even the first few days after vaccination (Rose, 2021), it seems likely that the acceleration of cancer progression following vaccines would be a difficult signal to recognize. Furthermore, most people do not expect cancer to be an adverse event that could be caused by a vaccine, and hence they fail to enter a report when cancer develops shortly after vaccination.
They should have stopped right there, but they couldn’t resist continuing:
However, as we have outlined in our paper, if the mRNA vaccinations are leading to widespread dysregulation of oncogene controls, cell cycle regulation, and apoptosis, then VAERS reports should reflect an increase in reports of cancer, relative to the other vaccines, even if the numbers are small. The experiment demonstrating impairment of DNA repair mechanisms by SARS-CoV-2 spike protein in an in vitro study provides compelling evidence that the vaccines could accelerate the rate of DNA mutations, increasing cancer risk (Jiang and Mei, 2021).
Again, Seneff et al. were right at first before they went wrong. Cancer is the culmination of a process that, in general, takes years, from the initial insult that resulted in cellular transformation to the development of a cancerous tumor detectable by symptoms, physical exam, or screening tests. As I discussed before when antivaxxers did a similar thing with another database to try to blame cancer on COVID-19 vaccines, even after radiation exposure from an atomic bomb, the increased risk of cancer from such a carcinogenic exposure is too long for this to make sense. For leukemias, it’s about two years before the earliest signals can be seen. (The vaccines have only been widely available for less than a year and a half). For solid cancers, the lag time is about 10 years. The increased risks from radiation from the atomic bombs dropped on Hiroshima and Nagasaki, especially those for solid cancers, were most easily detected after 30 years and remain over a person’s lifetime. Basically, the authors concede (sort of) that it’s too early to detect an increased risk of cancer from COVID-19 vaccines but then pivot to a hand wave that says, “But look at our mechanisms!” Never mind that the mechanisms were highly speculative to begin with and unproven.
I could go on about the VAERS section, but Prof. Morris did a fine job with it already, and I only wanted to harp on the cancer part because I’m a cancer surgeon and biologist myself. Remember, VAERS is a database to which anyone can contribute anything as a report of an “adverse event” after vaccination, and antivaxxers have been gaming VAERS since the 1990s. It’s a problem that has only gotten so much worse since the pandemic hit. VAERS is useful as an early warning system, but only if you know how to use it, a skill that involves knowing the base rate of the adverse events reported in the population.
Disinformation now and disinformation then
I started this post by pointing out how bogus scientific “review” articles are a long-time favorite technique of spreading antivaccine misinformation. In fact, they are a favorite tool of spreading science denial of all kinds, particularly of evolution and climate science, but I know antivaccine science denial better than I know those other forms, which is why I’ll stick to a couple of examples from the past. One dates back to 2011, when a Helen Ratajczak published an article in the Journal of Immunotoxicology titled “Theoretical aspects of autism: Causes–A review“. This review article was picked up by Sharyl Attkisson, an antivax reporter who has now become an all-around conspiracy theorist and COVID-19 denialist, to promote the claim that vaccines cause autism. As an aside, Attkisson’s report produced the still hilarious misspelling that those of us who have been following the antivaccine movement a long time still bring up to this day, “homologous recombinaltion tiniker.” She meant to write homologous recombination, the process by which DNA with a highly homologous (similar) sequence to a sequence in the genome can integrate itself in that spot, but the misspelling lives on.
Basically, Ratajczak’s claim was that DNA from the “fetal cells” used to manufacture some vaccines could get into the brain, undergo homologous recombination with the DNA of neurons, and produce “foreign” proteins (fusions of “self” proteins plus the fetal protein) that would result in autoimmunity and cause autism. That’s it. That’s the idea, which is incredibly implausible. To do what Dr. Ratajczak claims, the minute amount of human fetal DNA in a vaccine would have to:
- Find its way to the brain in significant quantities.
- Make it into the neurons in the brain in significant quantities.
- Make it into the nucleus of the neurons in significant quantities.
- Undergo homologous recombination at a detectable level, resulting in either the alteration of a cell surface protein or the expression of a foreign cell surface protein that the immune system can recognize.
- Undergo homologous recombination in many neurons in such a way that results in the neurons having cell surface protein(s) altered sufficiently to be recognized as foreign.
That’s leaving aside the issue of whether autoimmunity in the brain or chronic brain inflammation is even a cause of autism, which is by no means settled by any stretch of the imagination. In fact, quite the opposite. It’s not at all clear whether the markers of inflammation sometimes reported in the brains of autistic children are a cause, a consequence, or merely an epiphenomenon of autism. In other words, Dr. Ratajczak’s hypothesis is incredibly implausible on the basis of what we know about molecular biology and human biology. It’s not quite homeopathy-level implausible, but nonetheless quite implausible.
Her review was useful in that it also listed another favorite “hypothesis” of antivaxxers from a decade ago, namely deficiencies in metal metabolism that predisposed children to autism when they were exposed to mercury (from vaccines, of course):
Defective metallothionein might be responsible for the greater amount of blood mercury found in autistic children compared to neurotypical controls (Desoto and Hitlan, 2007; Geier et al., 2010). Metallothionein plays an important role in the development and continued function of the immune response, in neuronal development, and in the detoxification of heavy metals. Many classic symptoms of autism may be explained by a metallothionein defect, including gastrointestinal (GI) tract problems, heightened sensitivity to toxic metals, and abnormal behaviors. Porphyrinuria in children with autism is considered a marker of heavy metal toxicity (Geier and Geier, 2006a; Nataf et al., 2006, 2008; Rossignal, 2007; Geier et al., 2009). Individuals with severe autism had increased mercury-intoxication-associated urinary porphyrins (Geier et al., 2009).
Again, there was (and still is) no good scientific evidence to support the plausibility of these hypotheses. I could list a whole slew of papers trying to link various metabolic processes to autism via vaccine “injury” but will spare you. I’ll also note that the Hannah Poling case was a huge driver of papers claiming to link mitochondrial disorders to autism via vaccine injury. The idea was that mitochondrial disorders make a child susceptible to neurologic damage due to fevers due to vaccines. But you know what causes fevers more effectively? Actual infections! That’s why it is highly recommended that children with mitochondrial diseases receive the full slate of childhood vaccines. And don’t even get me started on another highly speculative “mechanism” how vaccines could supposedly cause autism known as “microcompetition“.
One thing that distinguishes Ratajczak’s review from that of Seneff et al. is that Ratajczak discussed a number of non-crank hypotheses with actual science behind them (e.g., the association of certain gene mutations, increased paternal age, and more) along with her vaccine-autism causation pseudoscience, the better to disguise the antivaccine pseudoscience. Seneff et al. could have learned from that, but apparently they didn’t. The idea was the same, though, to get a “review article” into the scientific literature to provide scientific-sounding highly speculative talking points that antivaxxers could use to blame autism on vaccines, exactly the same thing that Seneff et al. accomplished.
Finally, Seneff et al. was published in Food and Chemical Toxicology, a journal by a large scientific publishing house, Elsevier. I note that it’s the same journal that published Gilles-Eric Séralini’s awful GMO study that was ultimately retracted. More importantly, it is a journal that had no business publishing a review article like this, given that it’s not a journal dedicated to vaccines, infectious disease, epidemiology, or other relevant specialties. It is a toxicology journal, but it’s a stretch for it to cover alleged adverse reactions from COVID-19 vaccines and a whole lot of Gish galloping about potential biological mechanisms for those complications. One has to wonder why Jose Luis Domingo, who is listed as the editor who handled this review, let it pass and why the peer reviewers didn’t reject it.
I think I know why. The most charitable explanation is likely twofold. First, COVID-19 articles, particularly ones claiming adverse reactions from vaccines, bring clicks, and editors want to publish them. More importantly, though, an explanation that doesn’t require any sort of conflict of interest or nefarious motivation on the part of the journal editor is that neither journal editors nor peer reviewers recognize misinformation and disinformation. They therefore reviewed Seneff et al. as though it were a serious attempt at a scientific review, not recognizing the Gish galloping. Even giving them that benefit of the doubt, though, I have a hard time not faulting them for failing to recognize the highly speculative nature of the claims, the obvious misuse of VAERS, and the even more highly selective citation (and self-citation) of papers that don’t really support the hypotheses proposed, at least not without a lot of contortions of logic and biology. These were not subtle flaws.
As professions, we scientists and physicians could in the past be blissfully oblivious to misinformation and disinformation. No longer. If we don’t get our acts together to recognize them, the result will be many more “reviews” like this weaponized to attack public health. Actually, it’s already too late, but maybe the deluge can be at least reversed and the cranks forced to publish this nonsense where they used to: In bottom-feeding journals and on their own websites, rather than in Elsevier journals.